
Cruciate repairs

I completed my first cruciate repair back in 1996 using a technique that was popular then with what was called an 'Over the Top' repair. We used material from the dog's body to create a ligament that was threaded through the joint and re-attached.
It sounds pretty logical and some surgeons still get good success from it but too many do not.
We then moved on to using synthetic materials to mimic the ligament around the joint and some of these versions are still very popular and have been updated with more secure materials, and better techniques of attachment.
After I completed my additional surgical qualifications in 2005, I moved on to some of the techniques changing the shape of the joint and will now choose these versions whenever I can.
Some surgeons stick to one of the techniques only but I am not terribly loyal to any of them.
None of the techniques are perfect and surgeons will argue for years about which is the best version.
I will generally look at the patient's shape, size, age and lifestyle, and then consider my budget in order to identify what I believe to be most suited.
One of there recent innovations as was TTA.
This technique was mathematically modelled and involves cutting the shin bone, changing the position of the patellar ligament. This connect the powerful thigh muscles to the shun bone via the kneecap.
It works well, and gets good results, with a low complication rate.
I started these from around 2007.
Whilst I like it, it is no longer my favourite !
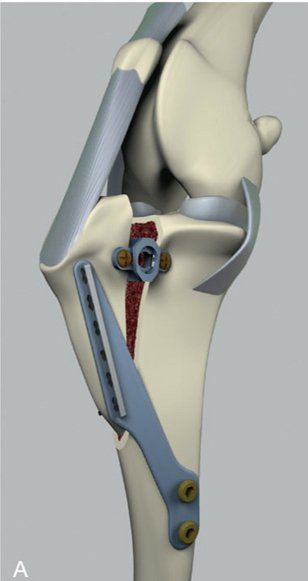
Graphic showing a TTA - Tibial Tuberosity Advancement
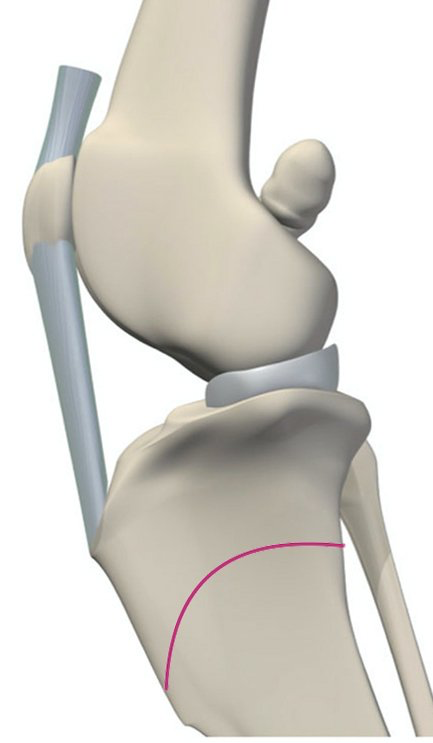
The graphic on the left is a Closing wedge Tibial Plateau Levelling Osteotomy or TPLO..
We cut the shin bone, take a small wedge out - the blue shaded area, and then rock the top downward and then put it back together.
This has the effect of altering the slope on the top of the shin bone and reducing the forces that are trying to force the thigh bone backwards over the surface of the shin bone.
It can be utilised on many different shapes and sizes of dog.
Other versions have been introduced that have advantages over the original but the original version is still incredibly successful..
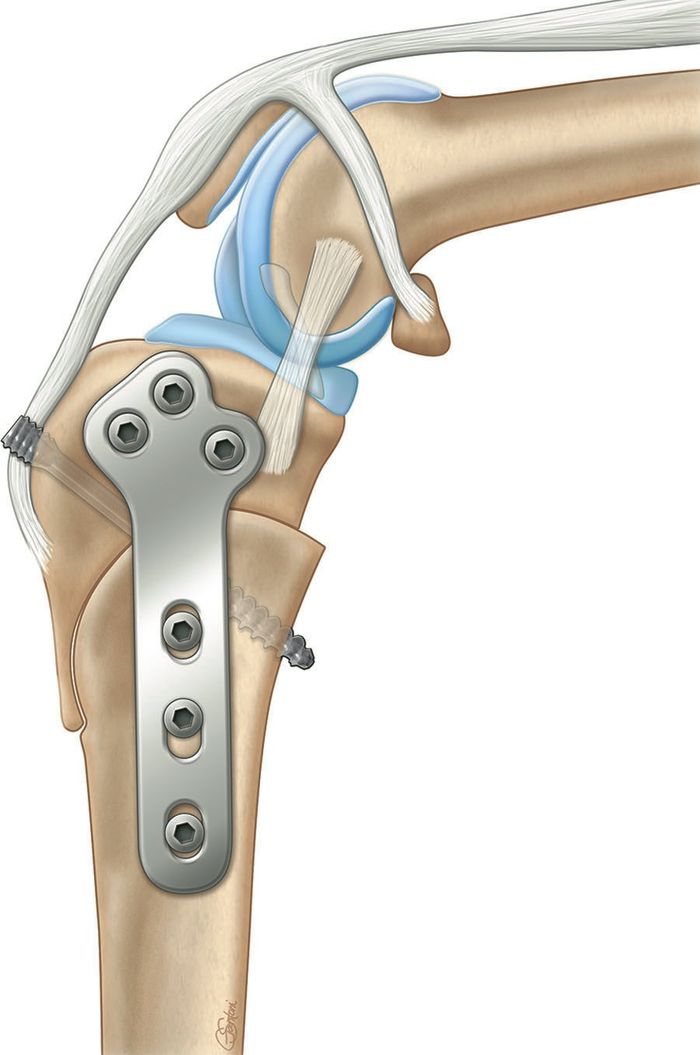
The CORA based Levelling Osteotomy or CBLO is one of the latest versions of surgery.
It has been designed by a Don Hulse, a surgeon from Texas and then developed with another couple of well known surgeons who all have great track records of thoroughly investigating problems, and identifying solutions.
It took a fresh look at the problem and the solutions by comparing it to deformities whereby bones fail to grow in the correct way, and joints then take up the wrong angles.
It has been shown to be superior in many respects to other versions, but may never be as popular.
Having visited Texas A&M University to watch Professor Hulse in action, reading his the papers evaluating its performance, I have come to see this version of surgery as being one of the best devised to date.


Once I take a look at the patient's x-rays I can take a look at what might be more appropriate and suitable.
Cost often does come into the equation of decision making, and whilst we would all prefer that this was not the case, we can usually consider the best result when finances also cause us a headache.

And there's more....
Within the joint, there is a structure called the meniscus.
Us humans often manage to damage this structure twisting our knee without necessarily damaging the cruciate.
It is a common injury for footballers and often then described as 'cartilage surgery'.
The structure is packed with nerve cells but limited blood supply. Consequently it doesn't heal well even if it can be sutured back together. Once torn, it can be really painful, indeed Professor Hulse described it as feeling like he'd broken his leg.
This can get damaged when the cruciate ruptures, or if unlucky, then a number of patients will unfortunately squash them and tear them following surgery - and sometimes, this can be months or even years after surgery.
We do try & deal with this at surgery but it is an important structure in the joint - like having a soft saucer cushioning a cup above it. If we can leave it to its job, that is preferable, but when damaged, or if likely to get damaged, we have to consider our approach during surgery.